H5N1
|
|
WHO pandemic phases
- Low risk
- New virus
- Self limiting
- Person to person
- Epidemic exists
- Pandemic exists
|
H5N1 flu refers to the transmission and
infection of
H5N1. H5N1 flu is a concern due to the
global spread of H5N1 that constitutes a pandemic threat.
This article is about the transmission of the H5N1 virus,
infection by that virus, the resulting symptoms of that
infection (having or coming down with influenza or more specifically
avian flu or even more specifically H5N1 flu which can
include
pneumonia), and the medical response including
treatment.
Infected birds pass on H5N1 through their saliva, nasal
secretions, and feces. Other birds may pick up the virus
through direct contact with these excretions or when they
have contact with surfaces contaminated with this material.
Because migratory birds are among the carriers of the H5N1
virus it may spread to all parts of the world. Past
outbreaks of avian flu have often originated in crowded
conditions in southeast and east Asia, where humans, pigs,
and poultry live in close quarters. In these conditions a
virus is more likely to mutate into a form that more easily infects humans.
The majority of H5N1 flu cases have been reported in
southeast and east Asia. Once an outbreak is detected, local
authorities often order a mass slaughter of birds or animals
affected. If this is done promptly, an outbreak of avian flu
may be prevented. However, the United Nations (UN) World
Health Organization (WHO) has expressed concern that not all
countries are reporting outbreaks as completely as they
should. China, for example, is known to have initially
denied past outbreaks of severe acute respiratory syndrome (SARS)
and HIV, although there have been some signs of improvement regarding
its openess in recent months, particularly with regard to
H5N1.
H5N1 infections in humans are generally caused by bird to
human transmission of the virus. Until May 2006, the WHO
estimate of the number of human to human transmission had
been "two or three cases". On May 24, 2006, Dr. Julie L.
Gerberding, director of the United States Centers for
Disease Control and Prevention in Atlanta, estimated that
there had been "at least three." On May 30, Maria Cheng, a
WHO spokeswoman, said there were "probably about half a
dozen," but that no one "has got a solid number."[1] A few
isolated cases of suspected human to human transmission
exist.[2] with the latest such case in June 2006 (among
members of a family in Sumatra).[3] No pandemic strain of H5N1 has yet been found. The key
point is that, at present, "the virus is not spreading
efficiently or sustainably among humans."[4]
There is also concern, although no definitive proof, that
other animals — particularly cats — may be able to act as a
bridge between birds and humans. So far several cats have
been confirmed to have died from H5N1 and the fact that cats
have regular close contact with both birds and humans means
monitoring of H5N1 in cats will need to continue.
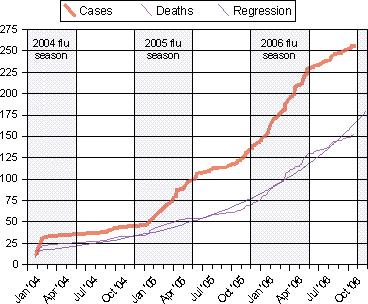
Cumulate Human Cases of and Deaths from
H5N1
As of
October 31, 2006
 |
| |
Notes:
- Source
WHO
Confirmed Human Cases of H5N1
- "[T]he incidence of human cases
peaked, in each of the three years in which
cases have occurred, during the period roughly
corresponding to winter and spring in the
northern hemisphere. If this pattern continues,
an upsurge in cases could be anticipated
starting in late 2006 or early 2007."
Avian influenza – epidemiology of human H5N1
cases reported to WHO
- The
regression curve for deaths is y = a + ek x,
and is shown extended through the end of
November, 2006.
H5N1 vaccines for chickens exist and are sometimes used,
although there are many difficulties that make deciding if
it helps more or hurts more especially difficult. H5N1
pre-pandemic vaccines exist in quantities sufficient to
inoculate a few million people[5]
and might be useful for priming to "boost the immune
response to a different H5N1 vaccine tailor-made years later
to thwart an emerging pandemic".[6]
H5N1 pandemic vaccines and technologies to rapidly create
them are in the
H5N1 clinical trials stage but can not be verified as
useful until after there exists a pandemic strain.
Avian flu in birds
According to Avian Influenza by Timm C. Harder and
Ortrud Werner:
- Following an incubation period of usually a few days
(but rarely up to 21 days), depending upon the
characteristics of the isolate, the dose of inoculum,
the species, and age of the bird, the clinical
presentation of avian influenza in birds is variable and
symptoms are fairly unspecific.[7]
Therefore, a diagnosis solely based on the clinical
presentation is impossible. The symptoms following
infection with low pathogenic AIV may be as discrete as
ruffled feathers, transient reductions in egg production
or weight loss combined with a slight respiratory
disease.[8]
Some LP strains such as certain Asian H9N2 lineages,
adapted to efficient replication in poultry, may cause
more prominent signs and also significant mortality.[9][10]
In its highly pathogenic form, the illness in chickens
and turkeys is characterised by a sudden onset of severe
symptoms and a mortality that can approach 100% within
48 hours.[11][12]
Poultry farming practices have changed due to H5N1:
- killing millions of poultry
-
vaccinating poultry against
bird flu
- vaccinating poultry workers against
human flu
- limiting travel in areas where H5N1 is found
- increasing farm hygiene
- reducing contact between
livestock and wild birds
- reducing open-air
wet markets
- limiting workers contact with
cock fighting
- reducing purchases of live fowl
- improving veterinary
vaccine availability and cost.
[13]
For example, after nearly two years of using mainly
culling to control the virus, the
Vietnamese government in 2005 adopted a combination of mass poultry vaccination,
disinfecting, culling, information campaigns and bans on
live poultry in cities.[14]
Webster et al write
- Transmission of highly pathogenic H5N1 from domestic
poultry back to migratory waterfowl in western China has
increased the geographic spread. The spread of H5N1 and
its likely reintroduction to domestic poultry increase
the need for good agricultural vaccines. In fact, the
root cause of the continuing H5N1 pandemic threat may be
the way the pathogenicity of H5N1 viruses is masked by
cocirculating influenza viruses or bad agricultural
vaccines."[15]
Dr. Robert Webster explains: "If you use a good vaccine
you can prevent the transmission within poultry and to
humans. But if they have been using vaccines now [in China]
for several years, why is there so much bird flu? There is
bad vaccine that stops the disease in the bird but the bird
goes on pooping out virus and maintaining it and changing
it. And I think this is what is going on in China. It has to
be. Either there is not enough vaccine being used or there
is substandard vaccine being used. Probably both. It’s not
just China. We can’t blame China for substandard vaccines. I
think there are substandard vaccines for influenza in
poultry all over the world."
[16] In response to the
same concerns, Reuters reports Hong Kong infectious disease
expert Lo Wing-lok saying, "The issue of vaccines has to
take top priority," and Julie Hall, in charge of the WHO's
outbreak response in China, saying China's vaccinations
might be masking the virus."
[17] The BBC reported
that Dr Wendy Barclay, a virologist at the University of
Reading, UK said: "The Chinese have made a vaccine based on
reverse genetics made with H5N1 antigens, and they have been
using it. There has been a lot of criticism of what they
have done, because they have protected their chickens
against death from this virus but the chickens still get
infected; and then you get drift - the virus mutates in
response to the antibodies - and now we have a situation
where we have five or six 'flavours' of H5N1 out there."
[18]
Transmission by wild birds
(waterfowl)
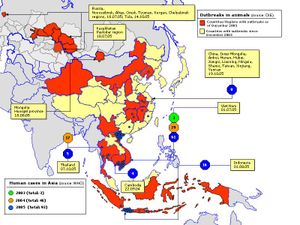
The spread of avian influenza in the eastern
hemisphere.
According to the
United Nations FAO: there is no denying the fact that wild
water fowl most likely play a role in the avian influenza
cycle and could be the initial source for AI viruses, which
may be passed on through contact with resident water fowl or
domestic poultry, particularly domestic ducks. The virus
undergoing mutations could circulate within the domestic and
possibly resident bird populations until HPAI arises. This
new virus is pathogenic to poultry and possibly to the wild
birds that it arose from. Wild birds found to have been
infected with HPAI were either sick or dead. This could
possibly affect the ability of these birds to carry HPAI for
long distances. However, the findings in Qinghai Lake-China,
suggest that H5N1 viruses could possibly be transmitted
between migratory birds. Additionally, the new outbreaks of
HPAI in poultry and wild birds in Russia, Kazakhstan,
Western China and Mongolia may indicate that migratory birds probably act
as carriers for the transport of HPAI over longer distances.
Short distance transmission between farms, villages or
contaminated local water bodies is likewise a distinct
possibility. The AI virus has adapted to the environment in
ways such as: 1) the use of water for survival and to spread
2) has evolved in a reservoir (ducks) strictly tied to
water. The water in turn influences movement, social
behaviour and migration patterns of water bird species. It
is therefore of great importance to know the ecological
strategy of influenza virus as well, in order to fully
understand this disease and to control outbreaks when they
occur. There remains a body of data and analysis missing on
the collection and detection of HPAI viruses in wild birds.
Finding HPAI viruses in wild birds may be a rare event, but
if the contact with susceptible species occurs it can cause
an outbreak at the local level or in distant areas.
[19]
Prevention
The current method of prevention in animal populations is
to destroy infected animals, as well as animals suspected of
being infected. In southeast
Asia, millions of domestic birds have been slaughtered
to prevent the spread of the virus.
The probability of a "humanized" form of H5N1 emerging
through genetic recombination in the body of a human
co-infected with H5N1 and another influenza virus type (a
process called reassortment) could be reduced by influenza
vaccination of those at risk for infection by H5N1. It
is not clear at this point whether vaccine production and
immunization could be stepped up sufficiently to meet this
demand. Additionally, vaccination of only humans would not
address the possibility or reassortment in pigs, cats, or
other mammal hosts.
If an outbreak of pandemic flu does occur, its spread
might be slowed by increasing hygiene in aircraft, and by
examining airline cabin air filters for presence of H5N1
virus.
The
American
Centers for Disease Control and Prevention advises
travelers to areas of Asia where outbreaks of H5N1 have
occurred to avoid poultry farms and animals in live food
markets
[20]. Travelers should
also avoid surfaces that appear to be contaminated by feces
from any kind of animal, especially poultry.
There are several H5N1 vaccines for several of the avian
H5N1 varieties. H5N1 continually mutates rendering them, so
far for humans, of little use. While there can be some
cross-protection against related flu strains, the best
protection would be from a vaccine specifically produced for
any future pandemic flu virus strain. Dr. Daniel Lucey,
co-director of the Biohazardous Threats and Emerging
Diseases graduate program at Georgetown University has made
this point, "There is no H5N1 pandemic so there can be no
pandemic vaccine." [21] However, "pre-pandemic vaccines"
have been created; are being refined and tested; and do have
some promise both in furthering research and preparedness
for the next pandemic [22]. Vaccine manufacturing companies
are being encouraged to increase capacity so that if a
pandemic vaccine is needed, facilities will be available for
rapid production of large amounts of a vaccine specific to a
new pandemic strain.
It is not likely that use of
antiviral drugs could prevent the evolution of a
pandemic flu virus.
[23]
Environmental survival
Avian flu virus can last forever at a temperature dozens
of degrees below freezing, as is found in the northern most
areas that migratory birds frequent.
Heat kills
H5N1 (i.e. inactivates the virus):
- Over 30 days at 0şC (32.0şF) (over one month at
freezing temperature)
- 6 days at 37şC (98.6şF) (one week at human body
temperature)
- 30 minutes 60şC (140.0şF) (half hour at a
temperature that causes first and second degree burns in
humans in ten seconds)[24]
Inactivation of the virus also occurs under the following
conditions:
- Acidic pH conditions
Presence of oxidizing agents such as sodium dodecyl
sulfate, lipid solvents, and B-propiolactone
Exposure to disinfectants: formalin, iodine compounds
[25]
Incubation
The human incubation period of avian influenza A (H5N1)
is 2 to 17 days[26].
Once infected, the virus can spread by cell-to-cell contact,
bypassing receptors. So even if a strain is very hard to
initially catch, once infected, it spreads rapidly within a
body.[27]
Symptoms
Avian influenza HA bind alpha 2-3
sialic acid receptors while human influenza HA bind
alpha 2-6 sialic acid receptors. Usually other differences
also exist. There is as yet no human form of H5N1, so all
humans who have caught it so far have caught avian
H5N1.
Human flu symptoms usually include fever, cough, sore
throat, muscle aches, conjunctivitis and, in severe cases,
severe breathing problems and pneumonia that may be fatal.
The severity of the infection will depend to a large part on
the state of the infected person's immune system and if the victim has been exposed to the
strain before, and is therefore partially immune. No one
knows if these or other symptoms will be the symptoms of a
humanized H5N1 flu.
Highly pathogenic
H5N1 avian flu in a human is far worse, killing over 50% of
humans that catch it. In one case, a boy with H5N1
experienced diarrhea followed rapidly by a coma without developing respiratory or flu-like
symptoms.
[28]
There have been studies of the levels of cytokines in
humans infected by the H5N1 flu virus. Of particular concern
is elevated levels of tumor necrosis factor alpha (TNFα), a
protein that is associated with tissue destruction at sites
of infection and increased production of other cytokines.
Flu virus-induced increases in the level of cytokines is
also associated with flu symptoms including fever, chills,
vomiting and headache. Tissue damage associated with
pathogenic flu virus infection can ultimately result in
death [29]. The inflammatory cascade triggered by H5N1 has
been called a 'cytokine storm' by some, because of what
seems to be a positive feedback process of damage to the
body resulting from immune system stimulation. H5N1 type flu
virus induces higher levels of cytokines than the more
common flu virus types such as H1N1 [30] Other important
mechanisms also exist "in the acquisition of virulence in
avian influenza viruses" according to the CDC.[31]
The NS1
protein of the highly pathogenic avian H5N1 viruses
circulating in poultry and waterfowl in Southeast Asia is
currently believed to be responsible for the enhanced
proinflammatory cytokine response. H5N1 NS1 is characterized
by a single amino acid change at position 92. By changing
the amino acid from glutamic acid to aspartic acid,
researchers were able to abrogate the effect of the H5N1
NS1. This single amino acid change in the NS1 gene greatly
increased the pathogenicity of the H5N1 influenza virus.
In short, this one amino acid difference in the NS1
protein produced by the NS RNA molecule of the H5N1 virus is
believed to be largely responsible for an increased
pathogenicity (on top of the already increased pathogenicity
of its hemagglutinin type which allows it to grow in organs
other than lungs) that can manifest itself by causing a
cytokine storm in a patient's body, often causing pneumonia
and death.
Treatment
Neuraminidase inhibitors are a class of drugs that
includes
zanamivir and oseltamivir, the latter being licensed for
prophylaxis treatment in the United Kingdom. Oseltamivir
inhibits the influenza virus from spreading inside the
user's body [23]. It is marketed by Roche as Tamiflu. This
drug has become a focus for some governments and
organizations trying to be seen as making preparations for a
possible H5N1 pandemic. In August 2005, Roche agreed to
donate three million courses of o be deployed by the WHO to
contain a pandemic in its region of origin. Although Tamiflu
is patented, international law gives governments wide
freedom to issue compulsory licenses for life-saving drugs.
A second class of drugs, which include
amantadine and rimantadine, target the M2 protein, but are
ineffective against H5N1. Unlike zanamivir and oseltamivir,
these drugs are inexpensive and widely available and the WHO
had initially planned to use them in efforts to combat an
H5N1 pandemic. However, the potential of these drugs was
considerably lessened when it was discovered that farmers in
China have been administering amantadine to poultry with
government encouragement and support since the early 1990s, against international livestock regulations; the
result has been that the strain of the virus now circulating
in South East Asia is largely resistant to these medications
and hence significantly more dangerous to humans[32].
- However, recent data suggest that some strains of
H5N1 are susceptible to the older drugs. An analysis of
more than 600 H5N1 viruses collected in Southeast Asia
showed that most samples from China and Indonesia lacked
genetic characteristics signaling resistance to
amantadine, whereas most samples from Vietnam, Thailand,
and Cambodia had those characteristics. The report was
published by the Journal of Infectious Diseases. The new
WHO guidelines were drawn up by an international group
of clinicians with experience treating H5N1 patients,
along with other experts, at a meeting in late March.
The panel systematically reviewed and graded the
evidence for the drugs' effectiveness. Since no results
from controlled trials of medication use in H5N1 cases
are available, "Overall, the quality of the underlying
evidence for all recommendations was very low," the
138-page WHO report states. The evidence includes
results of lab and animal studies and indirect evidence
from studies of antiviral use in patients with seasonal
influenza. The recommendations are classified as
"strong" or "weak," depending on the quality of the
relevant evidence. The WHO says that if a patient has a
confirmed or strongly suspected H5N1 case and NIs are
available, "Clinicians should administer oseltamivir
treatment (strong recommendation); zanamivir might be
used as an alternative (weak recommendation)."
Oseltamivir comes in capsule form, whereas zanamivir is
taken with an inhaler. The WHO says zanamivir has lower
bioavailability outside the respiratory tract than
oseltamivir, but it may be active against some strains
of oseltamivir-resistant H5N1 virus.[33]
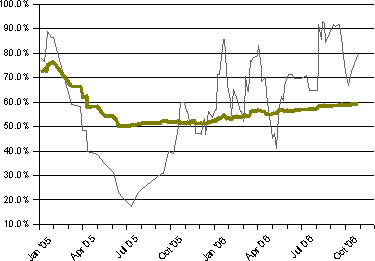
Mortality rate
- The thin line represents average
mortality of recent cases. The thicker line
represents mortality averaged over all cases.
- According to WHO: "Assessment of
mortality rates and the time intervals between
symptom onset and hospitalization and between
symptom onset and death suggests that the
illness pattern has not changed substantially
during the three years."[2]
A strain of H5N1 killed chickens in 1959 in Scotland and
turkeys in 1991 in England. This strain was "highly
pathogenic" (deadly to birds) but caused neither illness nor
death in humans.[34] "The precursor of the H5N1 influenza
virus that spread to humans in 1997 was first detected in
Guangdong, China, in 1996, when it caused a moderate number
of deaths in geese and attracted very little attention."
[35] In 1997, in Hong Kong, 18 humans were infected and 6 died in the
first known case of H5N1 infecting humans.
[36] H5N1 had
evolved from a zero mortality rate to a 33% mortality rate.
By 2003 H5N1 infection was detected in three flocks in
the
Republic of Korea.
This strain caused asymptomatic infections in humans and has
died out, meaning that its low mortality level is no more
relevant than the 1959 strain's low mortality rate.[37]
[38] The
apparently extinct strain that caused Vietnam's human deaths
from H5N1 in 2003, 2004 and 2005 also had a lower case
mortality rate than the currently existing strains.[38]
Changes are occurring in H5N1 that are increasing its
pathogenicity in mammals.[39]
In 2005, 42 of 97 people confirmed by the WHO to be
infected with H5N1 died -- or 43%. From January 1, 2006 to
October 31, 2006, the case fatality ratio has been higher,
with 74 deaths among 109 WHO-confirmed cases [40]-- or 68%.
This has been interpreted by some to mean that the virus
itself is becoming more deadly over time. [41] The global
case fatality ratio is, nonetheless, a crude summary of a
complex situation with many contributing factors. In
particular, if an influenza pandemic arises from one of the
currently circulating strains of Asian lineage HPAI A(H5N1),
the mortality rates for the resulting human adapted
influenza strain cannot be predicted with any
confidence.
H5N1 is currently much better adapted to birds than to
other hosts, which is why the disease it causes is called a
bird flu. No pandemic strain of H5N1 has yet been found. The
precise nature and extent of the genetic alterations that
might change one of the currently circulating avian flu
strains into a human flu strain cannot be known in advance.
While many of the current H5N1 strains circulating in birds
can generate a dangerous cytokine storm in healthy adult humans
[42][43],
the ultimate pandemic strain might arise from a less-lethal
strain, or its current level of lethality might be lost in
the adaptation to a human host.
The global case fatality ratio looks only to the official
tally of cases confirmed by the WHO. It takes no account of
other cases, such as those appearing in press reports. Nor
does it reflect any estimate of the global extent of mild,
asymptomatic, or other cases which are undiagnosed,
unreported by national governments to the WHO, or for any
reason cannot be confirmed by the WHO. While the WHO's case
count is clearly the most authoritative, these unavoidable
limitations result in an unknown number of cases being
omitted from it. The problem of overlooked but genuine cases
is emphasized by occasional reports in which later serology
reveals antibodies to the H5N1 infection in the blood of
persons who were never known to have bird flu, and who then
are confirmed by the WHO only retroactively as "cases." Press reports of such cases,
often poultry handlers, have appeared in various countries.
The largest number of asymptomatic cases was recently
confirmed among Korean workers who had assisted in massive
culls of H5N1-infected poultry.[44]
This relatively benign Korean strain of H5N1 has died out,
and the remaining strains of H5N1 have a higher case
fatality rate in humans.
Unconfirmed cases have a potentially huge impact on the
case fatality ratio. This mathematical impact is
well-understood by epidemiologists, and is easy to see in
theory. For example, if for each confirmed case reported by
the WHO we assume that there has been another mild and
unreported case, the actual global number of cases would be
double the current number of
WHO-confirmed
cases. The fatality ratio for H5N1 infections would then be
calculated as the same number of deaths, but divided by a
doubled number for total cases, resulting in a hypothetical
death ratio of half the currently-reported fatality ratio.
Such a result would indicate to epidemiologists that the
world was confronting an H5N1 virus that is less-lethal than
currently assumed, although possibly one that was more
contagious and difficult to track.
A case-fatality ratio based on an accurate and
all-inclusive count of cases would be invaluable, but
unfortunately it is impossible to attain. The ability to
diagnose every case of H5N1 as it arises does not exist. A
few reported studies have attempted to gather preliminary
data on this crucial statistic, by carrying out systematic
blood testing of neighbors and contacts of fatal cases in
villages where there had been confirmed H5N1 fatalities.
This testing failed to turn up any overlooked mild cases.
[45]
[46] These methodical
studies of contacts provide significant evidence that the
high death rate among confirmed cases in the villages where
these studies were carried out cannot be simply attributed
to a wholesale failure to detect mild cases. Unfortunately,
these studies are likely to remain too few and sketchy to
define the complex situation worldwide regarding the
lethality of the varying H5N1 clades. The testing and
reporting necessary for mass serology studies to determine
the incidence of overlooked cases for each existing clade
and strain of H5N1 worldwide would be prohibitively costly.
Hence the precise allocation of infections by the various
H5N1 clades across the spectrum including lethal, serious,
mild, and asymptomatic cases is likely to remain unknown in
both humans and the hundreds of other species it can infect.
Scientists are very concerned about what we do know about
H5N1; but even more concerned about the vast amount of
important data that we don't know about H5N1 and its future
mutations.
A case fatality ratio of over 50% provides a grim
backdrop for the fact that the currently circulating H5N1
strains have certain genetic similarities with the Spanish
Influenza pandemic virus. In that pandemic, 50 million to
100 million people worldwide were killed during about a year
in 1918 and 1919
[47]. The highly lethal
second and third waves of the 1918 Spanish flu evolved
through time into toward a less virulent and more
transmissible human form. Although the overall fatality rate
for the Spanish Flu was at most 1% to 2% of the population,
the lethal waves of the Spanish Flu are not reported to have
emerged with anything like the over-50% case fatality ratio
observed to date in human H5N1 infection. Unfortunately, a
human H5N1 pandemic might emerge with initial lethality
resembling that over-50% case fatality now observed in
pre-pandemic H5N1 human cases, rather than with the
still-high 1-2% seen with the Spanish Flu or with the lower
rates seen in the two more recent influenza pandemics.[48]
Review of patient ages and outcomes reveals that H5N1
attacks are especially lethal in pre-adults and young
adults, while older victims tend to have milder attacks and
to survive.
[49] This is consistent
with the frequent development of a cytokine storm in the
afflicted.[50] Very few persons over 50 years of age died
after suffering a H5N1 attack. Instead, the age-fatality
curve of H5N1 influenza attacks in humans resembles that of
the 1918 Spanish pandemic flu, and is the opposite of the
mortality curve of seasonal flu strains, since seasonal
influenza preferentially kills the elderly and does not kill
by cytokine storm.
Another factor complicating any attempt to predict
lethality of an eventual pandemic strain is that many human
victims of the current H5N1 influenza have been blood
relatives (but rarely spouses) of other victims. This data
suggests that the victims' genetic susceptibility may have
played a role in the human cases registered to date.
Mortality rate in planning reports
Governments and other organizations at many levels and in
many places have produced "planning" reports that, among
other things, have offered speculation on the mortality rate
of an eventual H5N1 pandemic. One such report stated that
"over half a million Americans could die and over 2.3
million could be hospitalized if a moderately severe strain
of a pandemic flu virus hits the U.S."[51].
No one knew if "moderately severe" was an accurate guess or
not. A report entitled A Killer Flu?[52]
projected that, with an assumed (guessed) contraction rate
of just 25%, and with a severity rate as low as that of the
two lowest severity flu pandemics of the 1900s, a modern
influenza A pandemic would cause 180 thousand deaths in the
US, while a pandemic equaling the 1918 Spanish Flu in level
of lethality would cause one million deaths in the US.
Again, the report offered no evidence that an emerging H5N1
flu pandemic would be between these figures[53].
The current avian flu, in humans, is fatal in over 50% of
confirmed cases. Yet early projections like those above have
assumed that such a lethal avian strain would surely lose
genes contributing to its lethality in humans as it made the
adaptations necessary for ready transmission in the human
population. This optimistic assumption cannot be relied on,
as the WHO reported in November 2006. Initial outbreaks of
an H5N1 pandemic could rival the current lethality of over
50%.[54]
Further information necessary to make an accurate projection
of initial lethality of an H5N1 pandemic does not exist, as
no data was collected that could show the pre-pandemic
virulence in any potential flu strain until after the last
pandemic of the 20th Century. There is no basis for assuming
that an H5N1 pandemic will emerge with only the far lower
1-2% lethality rate of the Spanish Flu, once assumed to be a
worst case scenario. There exists no reliable prediction of
the mortality rate of an H5N1 pandemic, and it would be
irresponsible to confine planning to only optimistic
assumptions out of step with the currently observed case
fatality ratio.
Although marred by unrealistically low ranges of assumed
mortality, the earlier planning reports nevertheless show
convincingly that we are not prepared even for a
pandemic as severe as the milder pandemics of the past
century.[55],
let alone the much higher case fatality ratios seen more
recently.
Notes and references
- ^
Donald G. McNeil Jr.. "Human
Flu Transfers May Exceed Reports", New York
Times,
June 4, 2006.
- ^
"Seven
Indonesian Bird Flu Cases Linked to Patients",
Bloomberg, May 23, 2006.
- ^
WHO confirms human transmission< in Indonesian bird
flu cluster.
- ^
"Avian
influenza – situation in Indonesia – update 17",
WHO, June 6, 2006.
- ^
HHS has enough H5N1 vaccine for 4 million people.
CIDRAP (July 5, 2006).
- ^
Study supports concept of 2-stage H5N1 vaccination.
CIDRAP (October 13, 2006).
- ^
A.R. Elbers, G.
Kock and A. Bouma (2005). "Performance
of clinical signs in poultry for the detection of
outbreaks during the avian influenza A (H7N7)
epidemic in The Netherlands in 2003". Avian
Pathol 34.
- ^
I. Capua and F.
Mutinelli (2001). "Low pathogenicity (LPAI) and
highly pathogenic (HPAI) avian influenza in turkeys
and chicken". A Colour Atlas and Text on Avian
Influenza.
- ^
S. Bano S, K. Naeem
K, S.A. Malik (2003). "Evaluation
of pathogenic potential of avian influenza virus
serotype H9N2 in chicken". Avian Dis
47, Suppl.
- ^
C Li, K Yu, G TiaG,
D Yu, L Liu, B Jing, J Ping, H. Chen (2005). "Evolution
of H9N2 influenza viruses from domestic poultry in
Mainland China". Virology 340.
- ^
D.E. Swayne, D.L.
Suarez (2000). "Highly
pathogenic avian influenza". Rev Sci Tech
19.
- ^
Timm C. Harder and Ortrud Werner.
Avian Influenza. Influenza Report.
- ^
The Threat of Global Pandemics. Council on
Foreign Relations (June 16, 2005). Retrieved on
2006-09-15.
- ^
"Vietnam
to unveil advanced plan to fight bird flu",
Reuters, April 28, 2006.
- ^
Robert G. Webster et al (January, 2006).
"H5N1
Outbreaks and Enzootic Influenza". Emerging
Infectious Diseases. Retrieved on
2006-09-15.
- ^
"Expert:
Bad vaccines may trigger China bird flu",
MSNBC, December 30, 2005. Retrieved on
2006-09-15.
- ^
"China H5N1 outbreak puts vaccines under spotlight",
Reuters, March 19, 2006. Retrieved on
2006-09-15.
This reference is apparently no longer available
online via Reuters. It is available as of 21 August,
2006 at
[1]
- ^
Bird flu vaccine no silver bullet. BBC (February
22, 2006). Retrieved on
2006-09-15.
- ^
Wild birds and Avian Influenza. FAO. Retrieved
on
2006-09-15.
- ^
National Center for Infectious Diseases, Division of
Global Migration and Quarantine (March 24, 2005).
Interim Guidance about Avian Influenza A (H5N1) for
U.S. Citizens Living Abroad. Travel Notices.
U.S. Centers for Disease Control and Prevention.
Retrieved on 2006-10-27.
- ^
Jennifer Schultz. "Bird flu vaccine won't precede
pandemic", United Press International, November
28, 2005. Retrieved on 2006-10-27.
- ^
Promising research into vaccines includes:
- ^
a b
Oseltamivir (Tamiflu).
National Institutes of Health (January 13,
2000). Revised on January 10, 2001.
- ^
Hot Water Burn & Scalding Graph. Retrieved on
2006-09-15.
- ^
Avian flu biofacts. CIDRAP.
-
^ Full text article online:
The Writing
Committee of the World Health Organization (WHO)
Consultation on Human Influenza A/H5 (September 29,
2005). "Avian
Influenza A (H5N1) Infection in Humans".
New England Journal of Medicine 353:
1374-1385.
- ^
T Jacob John (November 12, 2005).
Bird Flu: Public Health Implications for India.
Economic and Political Weekly.
- ^
(February 17, 2005) "Fatal
Avian Influenza A (H5N1) in a Child Presenting with
Diarrhea Followed by Coma". New England
Journal of Medicine 352 (7): 686-691.
- ^
Robert G. Webster
and Elizabeth Jane Walker (2003). "Influenza:
The world is teetering on the edge of a pandemic
that could kill a large fraction of the human
population". American Scientist 91:
122.
- ^
M. C. Chan et al
(2005). "Proinflammatory
cytokine responses induced by influenza A (H5N1)
viruses in primary human alveolar and bronchial
epithelial cells". Respiratory Research
6.
- ^
Martin Hirst,
Caroline R. Astell, Malachi Griffith, Shaun M.
Coughlin, Michelle Moksa, Thomas Zeng et al
(December 2004). "Novel
Avian Influenza H7N3 Strain Outbreak, British
Columbia". Emerg Infect Dis.
- ^
Alan Sipress. "Bird
Flu Drug Rendered Useless: Chinese Chickens Given
Medication Made for Humans", Washington Post,
June 18, 2005.
- ^
"WHO
sees role for older antivirals in some H5N1 cases",
CIDRAP, May 22, 2006.
- ^
"Situation
(poultry) in Asia: need for a long-term response,
comparison with previous outbreaks", Disease
Outbreak News: Avian influenza A(H5N1), WHO,
March 2,
2004. Retrieved on
2006-10-27.
- ^
Robert G. Webster, Malik Peiris, Honglin Chen, and
Yi Guan (January 2006).
H5N1 Outbreaks and Enzootic Influenza. CDC.
Retrieved on
2006-10-28.
-
^ WHO
(October 28, 2005).
H5N1 avian influenza: timeline.
- ^
"Five
Koreans had H5N1 virus but no illness",
CIDRAP, September 21, 2006.
- ^
a b
WHO (August 18, 2006).
Antigenic and genetic characteristics of H5N1
viruses and candidate H5N1 vaccine viruses developed
for potential use as pre-pandemic vaccines.
Contains latest Evolutionary "Tree of Life" for H5N1
-
^ Chen H,
Deng G, Li Z, Tian G, Li Y, Jiao P, Zhang L, Liu Z,
Webster RG, Yu K. (2004). "The evolution of H5N1
influenza viruses in ducks in southern China".
Proc. Natl. Acad. Sci. U. S. A. 101 (28):
10452-10457.
PubMed.
Full Text
- ^
Cumulative Number of Confirmed Human Cases of Avian
Influenza A/(H5N1) Reported to WHO. WHO (October
31, 2006).
- ^
H5N1 Getting Deadlier. based on the article
Bird Flu Fatality Rate in Humans Climbs to 64% as
Virus Spreads.
- ^
Clinical study points to cytokine storm in H5N1
cases. CIDRAP News (September 11, 2006).
- ^
Menno D de Jong
et al (September 10, 2006). "Fatal
outcome of human influenza A (H5N1) is associated
with high viral load and hypercytokinemia".
Nature. Published online.
- ^
Five Koreans had H5N1 virus but no illness (Sep
21,2006). CIDRAP. Retrieved on 2006-08-23.
- ^
"Mild
H5N1 cases weren’t found missed in Cambodian
outbreak study", CIDRAP, March 27, 2006.
- ^
"Cambodian
study suggests mild H5N1 cases are rare",
CIDRAP, September 7, 2006.
- ^
The Threat of Pandemic Influenza: Are We Ready?
Workshop Summary (2005). NAP. Retrieved on
2006-08-21.
- ^
http://www.cbc.ca/cp/health/061102/x110210.html
- ^
Human Avian Influenza A(H5N1) Cases by Age Group and
Country.
- ^
"Immediate
Treatment Needed for Bird Flu Cases, Study Says",
New York Times, September 11, 2006.
- ^
Pandemic Flu Projection Says More Than Half Million
Could Die in U.S.. Senior Journal (June 24,
2005).
- ^
Healthy Americans Full report PDF.
- ^
A Dramatic Disconnect. Newsweek. estimates two
million dead in the US, for example
- ^
http://www.cbc.ca/cp/health/061102/x110210.html
- ^
Dr. Martin Meltzer of the Centers for Disease
Control, an expert on the societal impact of
diseases, warns that “There is no healthcare system
anywhere in the world that can cope with even a mild
pandemic like the one in 1968.” Meltzer MI, Lancet
Asia Forum, Singapore, May 2006
Further reading













{kind=link}