Rabies
Dogs
Rabies
|
?
Rabies virus |
|
Virus classification |
| Group: |
Group V ((-)ssRNA) |
| Order: |
Mononegavirales |
| Family: |
Rhabdoviridae |
| Genus: |
Lyssavirus |
| Species: |
Rabies virus |
|
Rabies (from a Latin word meaning rage) is a
viral disease that causes acute
encephalitis in
animals and people. It can affect most species of warm-blooded animals, but
is rare among non-carnivores. In unvaccinated humans, rabies is almost
invariably fatal once full-blown symptoms have developed, but post-exposure
vaccination can prevent symptoms from developing.
Transmission and symptoms
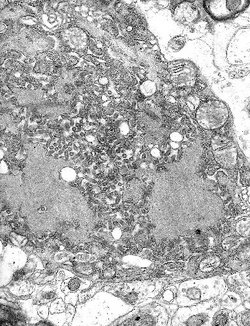 Micrograph with numerous rabies viruses (small dark-grey rod-like particles) and
Negri bodies, larger cellular inclusions typical of Rabies infection
Micrograph with numerous rabies viruses (small dark-grey rod-like particles) and
Negri bodies, larger cellular inclusions typical of Rabies infection
The stereotypical image of an infected ("rabid") animal is a "mad
dog" foaming at the
mouth, but cats,
ferrets,
raccoons,
skunks,
fox,
coyotes and
bats also become
rabid.
Squirrels,
chipmunks, other
rodents and
rabbits are
very seldom infected, perhaps because they would not usually survive an attack
by a rabid animal. Rabies may also be present in a so-called 'paralytic' form,
rendering the infected animal unnaturally quiet and withdrawn.
The virus is usually present in the
saliva of a
symptomatic rabid animal; the route of infection is nearly always by a bite. By
causing the infected animal to be exceptionally aggressive, the virus ensures
its transmission to the next host. Transmission has occurred via an
aerosol
through mucous membranes; transmission in this form may have happened in people
exploring caves populated by rabid bats. Transmission from person to person is
extremely rare, though it can happen through
transplant surgery (see below for recent cases), or even more rarely through
bites or kisses.
After a typical human infection by animal bite, the virus directly or
indirectly enters the peripheral nervous system. It then travels along the
nerves towards
the
central nervous system. During this phase, the virus cannot be easily
detected within the host, and vaccination may still confer cell-mediated
immunity to pre-empt symptomatic rabies. Once the virus reaches the
brain, it rapidly
causes an
encephalitis and symptoms appear. It may also inflame the spinal cord
producing
myelitis.
The period between infection and the first
flu-like symptoms is
normally 3-12 weeks, but can be as long as two years. Soon after, the symptoms
expand to
cerebral dysfunction,
anxiety,
insomnia,
confusion,
agitation, abnormal behaviour,
hallucinations, progressing to
delirium.
The production of large quantities of
saliva and
tears coupled with an inability to speak or swallow are typical during the later
stages of the disease; this is known as "hydrophobia".
Death almost invariably results 2-10 days after the first symptoms; the handful
of people who are known to have survived the disease were all left with severe
brain damage, with the recent exception of
Jeanna
Giese (see below).
The virus
The Rabies virus is a
Lyssavirus.
This genus of
RNA viruses also includes the
Aravan virus,
Australian bat lyssavirus,
Duvenhage virus,
European bat lyssavirus 1,
European bat lyssavirus 2,
Irkut virus,
Khujand virus,
Lagos bat virus,
Mokola
virus and
West Caucasian bat virus. Lyssaviruses have helical symmetry, so their
infectious particles are approximately cylindrical in shape. This is typical of
plant-infecting viruses; human-infecting viruses more commonly have cubic
symmetry and take shapes approximating
regular polyhedra.
The Lyssaviruses are the only viruses known to travel along the nerves after
infection. Biopsy
shows typical "Negri
bodies" in the infected neurons.
The Rabies virus has a bullet-like shape with a length of about
180 nm and a
cross-sectional diameter of about
75 nm. One
end is rounded or conical and the other end is planar or concave. The
lipoprotein envelope carries knob like spikes, composed og Glycoprotein G.
Spikes do not cover the planar end of the virion. Beneath the envelope is the
membrane or matrix (M) protein layer which may be invaginated at the planar end.
The core of the Virion consists of helically arranged ribonucleoprotein. The
genome is unsegmented linear negative sense RNA. Also present in the
nucleocapsid are RNA dependent RNA transcriptase and some structural proteins.
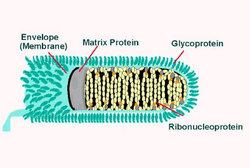 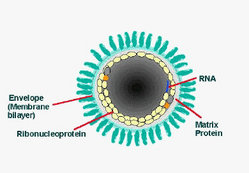
Longitudinal and cross-sectional schematic view of Rabies virus
Prevention
There is no known cure for symptomatic rabies, but it can be prevented by
vaccination, both in humans and other animals. Virtually every infection
with rabies was historically a death sentence, until
Louis
Pasteur developed the first rabies vaccination in
1886. Pasteur
demonstrated its effectiveness by treating
Joseph Meister, who had been bitten by a rabid dog.
Pasteur's vaccine consisted of a sample of the virus harvested from infected
(and necessarily dead) rabbits, which was weakened by allowing it to dry.
Similar nerve tissue-derived vaccines are still used today in developing
countries, and while they are much cheaper than modern cell-culture vaccines,
they are not as effective and carry a certain risk of neurological
complications.
Treatment after exposure (known as
post-exposure prophylaxis or "PEP") is highly successful in preventing the
disease if administered promptly, within 14 days after infection. In the United
States, the treatment consists of a regimen of one dose of
immunoglobulin and five doses of rabies vaccine over a 28-day period. Rabies
immunoglobulin and the first dose of rabies vaccine should be given as soon as
possible after exposure, with additional doses on days 3, 7, 14, and 28 after
the first. The vaccinations are relatively painless and are given in one's arm,
in contrast to previous treatments which were given through a large needle
inserted into the abdomen. In case of animal bites it is also helpful to remove,
by thorough washing, as much infectious material as soon as possible. Since the
development of effective human vaccines and immunoglobulin treatments the US,
death rate from rabies has dropped from 100 or more annually in the early 20th
century, to 1-2 per year, mostly caused by bat bites, which may go unnoticed by
the victim and hence untreated.
PEP is effective in treating rabies because the virus must travel from the
site of infection through the
peripheral nervous system (nerves in the body) before infecting the
central nervous system (brain and spinal cord) and glands to cause lethal
damage. This travel along the nerves is usually slow enough that vaccine and
immunoglobulin can be administered to protect the brain and glands from
infection. The amount of time this travel requires is dependent on how far the
infected area is from the brain: if the victim is bitten in the face, for
example, the time between initial infection and infection of the brain is very
short and PEP may not be successful.
Prevalence
Between 40,000 and 70,000 human beings die annually from rabies[citation
needed], with about 90% of those cases occurring in Asia. About 6
million people receive treatment annually after suspected exposure to rabies.
Every ten to fifteen minutes someone dies of rabies in the world.
Dog licensing, killing of stray dogs, muzzling and other measures contributed
to the eradication of rabies from
Great Britain in the early
20th
century. More recently, large-scale vaccination of cats, dogs and ferrets
has been successful in combatting rabies in some developed countries.
 A rabid dog, with saliva dropping out of the mouth
A rabid dog, with saliva dropping out of the mouth
Rabies virus survives in widespread, varied, rural wildlife reservoirs.
However, in Asia, parts of Latin America and large parts of Africa, dogs remain
the principal host. Mandatory vaccination of animals is less effective in rural
areas. Especially in developing countries, animals may not be privately owned
and their destruction may be unacceptable. Oral vaccines can be safely
distributed in baits, and this has successfully impacted rabies in rural areas
of France,
Ontario,
Texas,
Florida and
elsewhere. Vaccination campaigns may be expensive, and a cost-benefit analysis
can lead those responsible to opt for policies of containment rather than
elimination of the disease.
Rabies was once rare in the United States outside the
Southern states, but
raccoons in
the mid-Atlantic and northeast United States have been suffering from a rabies
epidemic since the
1970s, which is now moving westwards into
Ohio[1].
The particular variant of the virus has been identified in the southeastern
United States raccoon population since the
1950s, and is
believed to have traveled to the northeast as the result of infected raccoons
being among those caught and transported from the southeast to the northeast by
hunters attempting to replenish the declining northeast raccoon population
(Nettles VF, Shaddock JH, Sikes RK, Reyes CR. "Rabies in translocated raccoons".
Am J Public Health 1979;69:601-2.). As a result, urban residents of these
areas have become more wary of the large but normally unseen urban raccoon
population. It has become the common assumption that any raccoon seen in
daylight is infected; certainly the reported behavior of most such animals
appears to show some sort of illness, and autopsies usually confirm rabies.
Whether as a result of increased vigilance or just the normal avoidance reaction
to any animal not seen in the course of day to day life, such as a raccoon,
there have been no documented human rabies cases as a result of this variant.
This does not include, however, the greatly increasing rate of prophylactic
rabies treatments in cases of possible exposure, which numbered less than 100
persons annually in New York State before
1990, for instance,
but rose to approximately 10,000 annually between
1990 and
1995. At
approximately $1500 per course of treatment, this represents a considerable
public health expenditure. Raccoons do constitute approximately 50% of the
approximately 8,000 documented animal rabies cases in the United States (Krebs
JW, Strine TW, Smith JS, Noah DL, Rupprecht CE, Childs JE. "Rabies surveillance
in the United States during 1995". J Am Vet Med Assoc 1996;204:2031-44).
Domestic animals constitute only 8% of rabies cases (ibid.), but are
increasing at a rapid rate.
In the midwestern United States,
skunks are the
primary carriers of rabies, comprising 144 of the 237 documented animal cases in
1996. The most
widely distributed reservoir of rabies in the United States, however, and the
source of most human cases in the U.S., are
bats. Nineteen of the
22 human rabies cases documented in the United States between
1980 and
1997 have been
identified genetically as bat rabies. In many cases, victims are not even aware
of having been bitten by a bat, assuming that a small puncture wound found after
the fact was the bite of an insect or spider; in some cases, no wound at all can
be found, leading to the hypothesis that in some cases the virus can be
contracted via inhaling airborne
aerosols
from the vicinity of a bat or bats. For instance, the
Centers for Disease Control and Prevention warned on
May 9,
1997, that a woman
who died in October,
1996 in
Cumberland County, Kentucky and a man who died in December,
1996 in
Missoula County, Montana were both infected with a rabies strain found in
silver-haired bats; although bats were found living in the chimney of the
woman's home and near the man's place of employment, neither victim could
remember having had any contact with them. This inability to recognize a
potential infection, in contrast to a bite from a dog or raccoon, leads to a
lack of proper prophylactic treatment, and is the cause of the high mortality
rate for bat bites.
In case of an attack by a possibly rabid animal, most states in the United
States allow the killing of the attacking animal. Because a rabies diagnosis
requires that the brain tissue be preserved, it is recommended that rabid
animals are not to be shot in the head.
Australia
is one of the few parts of the world where rabies has never been introduced.
However, the Australian Bat Lyssavirus occurs naturally in both insectivorous
and fruit eating bats (flying foxes) from most mainland states. Scientists
believe it is present in bat populations throughout the range of flying foxes in
Australia.
Many territories, such as the
United Kingdom,
Ireland,
Hawaii, and
Guam, are free of
rabies (although there may be a very low prevalence of rabies among bats in the
UK; see below).
Recently publicised cases
Transmission by animal bites
Several recently publicised cases have stemmed from
bats, which are known
to be a vector for rabies.
The United Kingdom, which has stringent regulations on the importation of
animals, had also been believed to be entirely free from rabies until
1996 when a single
Daubenton's bat was found to be infected with a rabies-like virus usually
found only in bats - European Bat Lyssavirus 2 (EBL2). There were no more known
cases in the British Isles until
September 2002 when another Daubenton's bat tested positive for EBL2 in
Lancashire.
A bat conservationist who was bitten by the infected bat received post-exposure
treatment and did not develop rabies.
Then in
November 2002 David McRae, a Scottish bat conservationist from
Guthrie, Angus
who was believed to have been bitten by a bat, became the first person to
contract rabies in the United Kingdom since
1902. He died from
the disease on
November
24, 2002.
In October 2004
a wild female brown
bear killed one person and injured several others near the city of
Brasov, Central
Romania. The
bear was killed by hunters and diagnosed with rabies. More than one hundred
people were vaccinated afterwards.
In November 2004,
Jeanna
Giese, a 15-year old girl from
Fond du Lac,
Wisconsin,
became one of only six people known to have survived rabies after the onset of
symptoms, and the first known instance of a person surviving rabies without
vaccine treatment. All of the other five received
vaccination before symptoms developed. Giese's disease was already too far
progressed for the vaccine to help, and she was considered too weak to tolerate
it. Doctors at the Children's Hospital of Wisconsin in
Wauwatosa, a suburb of
Milwaukee, achieved her survival with an experimental treatment that
involved putting the girl into a drug-induced
coma, and
administering a cocktail of
antiviral drugs. Giese had symptoms of full-blown rabies when she sought
medical help, 37 days after being bitten by a
bat. Her family did
not seek treatment at the time because the bat seemed healthy. Jeanna regained
her weight, strength, and coordination while in the hospital. She was released
from the Children's Hospital of Wisconsin on
January 1,
2005.
Transmission through organ transplants
Rabies is known to have been transmitted between humans by
transplant surgery. The medical advisory web site Manbir Online notes "Under
no circumstances should a cornea be transplanted from a donor, who died of an
undiagnosed neurological disorder."
 A patient with rabies, 1959
A patient with rabies, 1959
Infections by
corneal transplant have been reported in Thailand (2 cases), India (2
cases), Iran (2 cases), the United States (1 case), and France (1 case). The CDC
documents the case in France in 1980. Details of two further cases of infection
resulting from corneal transplants were described in 1996.
In June 2004,
three organ recipients died in the
United States from rabies transmitted in the transplanted kidneys and liver
of an infected donor from
Texarkana.
There are bats near the donor's home, but he did not mention having been bitten.
The donor is now reported to have died of a cerebral hemorrhage, the culmination
of an unidentified neurological disorder, although recipients are said to have
been told the cause of death had been a car crash. Marijuana and cocaine were
found in the donor's urine at the time of his death, according to a report in
The New England Journal of Medicine. The surgeons
"thought he had suffered a fatal crack-cocaine overdose, which can
produce symptoms similar to those of rabies. 'We had an explanation for his
condition,' says Dr. Goran Klintmalm, a surgeon who oversees transplantation
at Baylor University Medical Center, where the transplants occurred. 'He'd
recently smoked crack cocaine. He'd hemorrhaged around the brain. He'd died.
That was all we needed to know.' ... Because of doctor-patient
confidentiality rules, doctors involved with this case would not talk about
it on the record, but a few did say that no cocaine was found in the donor's
blood, the E.R. doctors might have investigated his symptoms more
aggressively instead of assuming he had overdosed. (Because no autopsy was
done, doctors have not been able to establish whether the rabies or the
drugs actually killed him.)" (The New York Times Magazine, July 10,
2005)
In February 2005,
three German
patients in Mainz
and
Heidelberg were diagnosed with rabies after receiving various organs and
cornea transplants from a female donor. Two of the infected people died. Three
other patients who received organs from the woman have not yet shown rabies
symptoms. The 26 year old donor had died of heart failure in December 2004 after
consuming cocaine
and
ecstasy. In October 2004, she had visited
India, one of the
countries worst affected by rabies world-wide. Dozens of medical staff were
vaccinated against rabies in the two hospitals as a precautionary measure.
Associated Press reports that "Donated organs are never tested for rabies.
The strain detected in the victims' bodies is one commonly found in bats, health
officials said." According to CNN "Rabies tests are not routine donor screening
tests, Virginia McBride, public health organ donation specialist with the Health
Resources and Services Administration, said. The number of tests is limited
because doctors have only about six hours from the time a patient is declared
brain-dead until the transplantation must begin for the organs to maintain
viability."
Transport of pet animals between countries
Rabies is
endemic to many parts of the world, and one of the reasons given for
quarantine
periods in international animal transport has been to try to keep the disease
out of uninfected regions. However, most developed countries, pioneered by
Sweden, now allow unencumbered travel between their territories for pet animals
that have demonstrated an adequate immune response to rabies vaccination.
Such countries may limit movement to animals from countries where rabies is
considered to be under control in pet animals. There are various
lists of such countries. The United Kingdom has developed a list, and France
has a rather different list, said to be based on a list of the Office
International des Epizooties (OIE). The European Union has a harmonised
list. No list of rabies-free countries is readily available from OIE.
However, the recent spread of rabies in the northeastern United States and
further may cause a restrengthening of precautions against movement of possibly
rabid animals between countries.
Rabies and domestic skunks in the United States
Since there is no
USDA-approved vaccine or
quarantine
period for skunks,
pet skunks
are frequently
put down after biting a human.
The post-exposure rabies series must be administered to the bite victim
before the disease progresses too far. For that reason, there has to be a means
of determining whether the animal has rabies within a reasonable amount of time.
Without a recognized quarantine period for skunks, there is no way of knowing
how long to watch the animal for signs of the disease. That leaves no option but
to kill the skunk and test its brain cells for rabies.
Skunk owners have recently organized to campaign for USDA approval of a
vaccine and quarantine period for skunks in the United States.
See also
External links
Sources
Other links
Home | Up | Rabies | Raw Feeding
Dogs, made by MultiMedia | Free content and software
This guide is licensed under the GNU
Free Documentation License. It uses material from the Wikipedia.
|